Better Prenatal Testing Means More Abortion by Mark LeachLower termination rates still mean more Down syndrome abortions. A guest post by Mark Leach in response to my article in The Atlantic last week. Amy Julia Becker
Last week, Amy Julia had a column featured in The Atlantic discussing the advances made in prenatal testing for Down syndrome. Her editor titled it, "Better prenatal testing does not mean more abortion." The headline can be excused. It is a misunderstanding that equates termination rates with total number of abortions. To the contrary, current research shows there are more abortions due to prenatal diagnoses of Down syndrome than ever.
The historically-quoted termination rate of 90 percent has been criticized for some time. It is based on a 1999 study that reviewed rates quoted from different countries. The studies of the United States were from the late 1980's. The 90 percent figure, as it applies to America, was outdated almost at the time of publication.
In 2012, another review study was published that further undermined the 90 percent figure. It reviewed more recent studies of termination rates and has provided the justification for those critical of the 90 percent figure to disregard those who still quote that rate. The 2012 study, however, has its own limitations. Termination rates for Down syndrome in the United States are not tracked by most states. The 2012 study reviewed reports, the most recent of which were from just three states: Hawaii, California, and Maine. Termination rates varied widely, from Maine actually exceeding the 90 percent rate—93.3 percent—to the California study having the lowest reported rate of 61.4 percent.
The 2012 report quoted a range of rates to choose from: 67 percent, representing the weighted average of the three most current studies; 74.2 percent, the weighted average of all studies with unique populations; and, 85 percent from hospital-based studies. In the end, the best that could be concluded was that the 90 percent figure probably was not accurate; the termination rate was probably lower; but by how much is still not clear. What gets misunderstood is that the total number of abortions has increased, even with the lower rate, and for the same reason that the rate is lower.
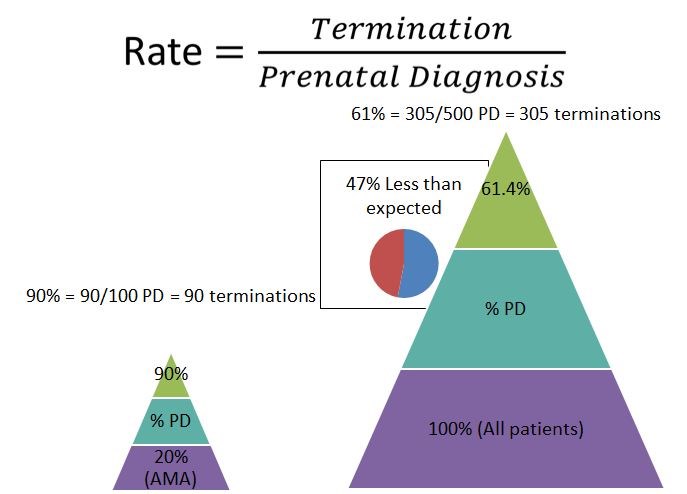
Rate and actual numbers of abortions are two different things. Rate is the result of dividing the number of expectant mothers who terminate following a prenatal diagnosis by the total number of expectant mothers with a prenatal diagnosis. This equation is illustrated in Figure 1.
Fig. 1. "AMA"=Advanced Maternal Age; "PD"=Prenatal Diagnosis; numbers used are for illustrative purposes.
As Figure 1 further illustrates, the 90 percent termination rate was based on data from a small population. When the 1999 study was published, the professional recommendation by the American Congress of Obstetricians & Gynecologists (ACOG) was that prenatal testing for Down syndrome should be offered to mothers 35 years of age or older. ACOG removed this age limit in 2007 so that all women are now offered prenatal testing. One of the reasons ACOG cited to justify its removal of the age limit was because 80 percent of all children born with Down syndrome are born to mothers under the age of 35.
The 90 percent termination rate, therefore, was of a population that represented only 20 percent of all Down syndrome pregnancies. With ACOG's removal of the age limit, 100 percent of all Down syndrome pregnancies are to be offered prenatal testing. This is both why the termination rate is lower and why there are more Down syndrome abortions than ever before.
If 90 percent of only 20 percent of the entire expectant population terminate following a prenatal diagnosis, that is a much smaller number than if even 61 percent (the lowest rate in the 2012 study) of 100 percent of the expectant population terminate. As illustrated in Figure 1, if, under the old ACOG guidelines, there were 100 patients with a prenatal diagnosis, a 90 percent termination rate would mean 90 abortions. But, under the current ACOG guidelines, if 500 women had a prenatal diagnosis (100 being 20 percent of 500), then a 61 percent termination rate would result in 305 abortions. With a larger base in the denominator, even if percentage-wise fewer women terminate, the actual number of women terminating is much more than when it was just 90 percent. The studies included in the 2012 study bear this out.
More mothers are having more children later in life than ever before. With the likelihood of having a child with Down syndrome directly correlating to the age of the mother, this means there should be more live births of children with Down syndrome than ever before. But this isn't the case.
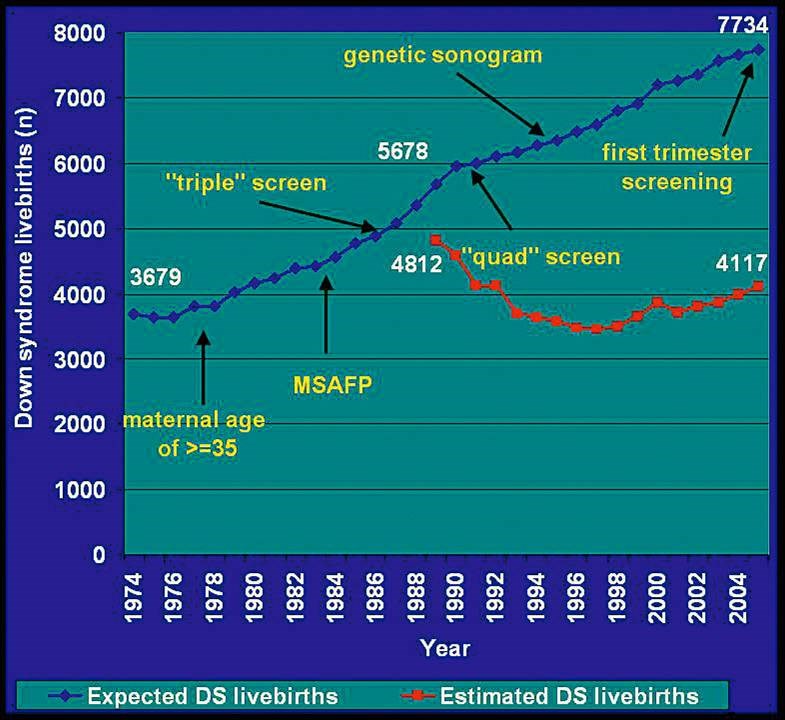
Instead, what researchers have found is that the number of live births of children with Down syndrome has remained the same as it was twenty years ago. One study estimated the number of births that would be expected with Down syndrome and then tracked the number of actual live births noting the introduction of prenatal tests as testing advanced over time. This study is shown in Figure 2. It shows how the number of live births has decreased slightly over time (the red line), but the number of expected births (the blue line) has grown with the average age of mothers increasing over time.
The same team of researchers updated their results in 2011 and found a 47 percent reduction between the number expected and the number of children with Down syndrome actually born. That same percentage was also found in the most recent California study.
The California study with the 61.4 percent termination rate expected there would be 1,326 births during its time frame, but instead just 711 births actually occurred, a difference of 47 percent. (See Figure 1). What is more is that the 2012 study included another California study. This other study was from 1997. It reported a termination rate from 1989 – 1991 of 88.3 percent. At this higher termination rate, though, the overall reduction rate between the number of Down syndrome pregnancies and those that were actually born was only 25.8 percent. So, in the same 2012 study were two studies of California: one from the late '80's reporting almost a 90 percent termination rate but a reduction of only 25.8 percent; and, another from 2005 – 2007 reporting a lower 61.4 percent termination rate, but almost a doubling of the reduction rate to 47 percent, a near halving of the next generation of babies born with Down syndrome.
The 2012 study reported a lower rate, but it included studies that showed the number of women who aborted was higher than when the rate was 90 percent. Commentators should avoid using the 90 percent termination rate when discussing prenatal testing in the United States. Instead, it should be appreciated that the most current research shows that for every baby with Down syndrome, there was another who was aborted.
Mark W. Leach is an attorney from Louisville, Kentucky with a Master's in Bioethics. Figure 1 is a slide he presented at the 2013 Annual Meeting for the South Atlantic Association of Obstetricians & Gynecologists. Mark blogs at www.downsyndromeprenataltesting.com.
Editor's note: I'm grateful to Mark, who has blogged here before about prenatal testing and Obamacare, for offering a nuanced response to my article for The Atlantic last week. And I agree with every word he wrote here. But I'm going to give myself the "last" word in saying that my hope remains that "better" prenatal testing in time will not simply mean prenatal testing for a wider swath of the population of pregnant women. My hope remains that "better" prenatal testing (as it relates to Down syndrome) is testing that offers more information about the real lives of families with children with Down syndrome from a social perspective and not just a medical one. My hope also remains that in time "better prenatal testing" will mean fewer abortions of babies with Down syndrome.