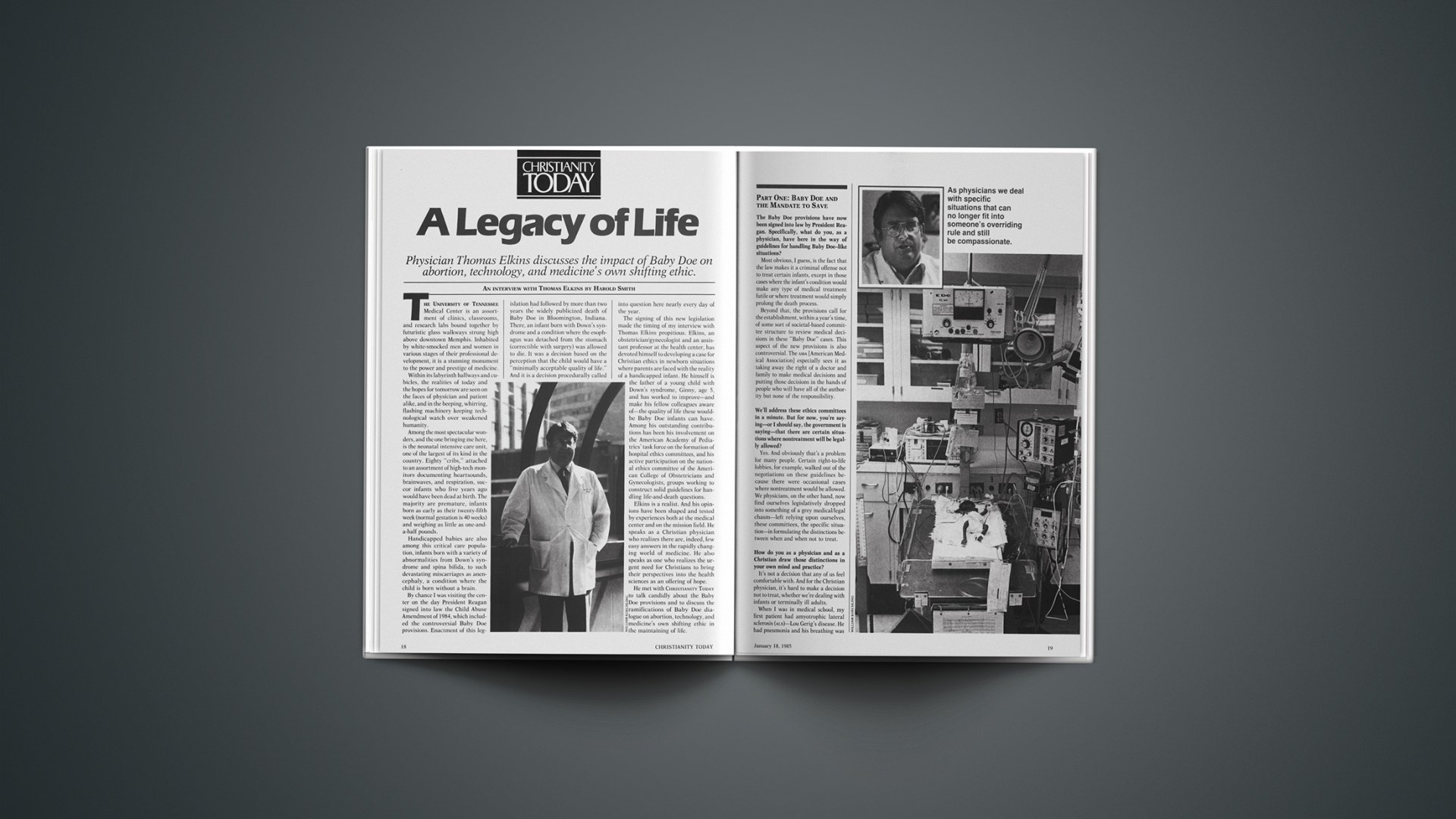

Physician Thomas Elkins discusses the impact of Baby Doe on abortion, technology, and medicine’s own shifting ethic.
The University of Tennessee Medical Center is an assortment of clinics, classrooms, and research labs bound together by futuristic glass walkways strung high above downtown Memphis. Inhabited by white-smocked men and women in various stages of their professional development, it is a stunning monument to the power and prestige of medicine.
Within its labyrinth hallways and cubicles, the realities of today and the hopes for tomorrow are seen on the faces of physician and patient alike, and in the beeping, whirring, flashing machinery keeping technological watch over weakened humanity.
Among the most spectacular wonders, and the one bringing me here, is the neonatal intensive care unit, one of the largest of its kind in the country. Eighty “cribs,” attached to an assortment of high-tech monitors documenting heartsounds, brainwaves, and respiration, succor infants who five years ago would have been dead at birth. The majority are premature, infants born as early as their twenty-fifth week (normal gestation is 40 weeks) and weighing as little as one-and-a-half pounds.
Handicapped babies are also among this critical care population, infants born with a variety of abnormalities from Down’s syndrome and spina bifida, to such devastating miscarriages as anencephaly, a condition where the child is born without a brain.
By chance I was visiting the center on the day President Reagan signed into law the Child Abuse Amendment of 1984, which included the controversial Baby Doe provisions. Enactment of this legislation had followed by more than two years the widely publicized death of Baby Doe in Bloomington, Indiana. There, an infant born with Down’s syndrome and a condition where the esophagus was detached from the stomach (correctible with surgery) was allowed to die. It was a decision based on the perception that the child would have a “minimally acceptable quality of life.” And it is a decision procedurally called into question here nearly every day of the year.
The signing of this new legislation made the timing of my interview with Thomas Elkins propitious. Elkins, an obstetrician/gynecologist and an assistant professor at the health center, has devoted himself to developing a case for Christian ethics in newborn situations where parents are faced with the reality of a handicapped infant. He himself is the father of a young child with Down’s syndrome, Ginny, age 5, and has worked to improve—and make his fellow colleagues aware of—the quality of life these would-be Baby Doe infants can have. Among his outstanding contributions has been his involvement on the American Academy of Pediatrics’ task force on the formation of hospital ethics committees, and his active participation on the national ethics committee of the American College of Obstetricians and Gynecologists, groups working to construct solid guidelines for handling life-and-death questions.
Elkins is a realist. And his opinions have been shaped and tested by experiences both at the medical center and on the mission field. He speaks as a Christian physician who realizes there are, indeed, few easy answers in the rapidly changing world of medicine. He also speaks as one who realizes the urgent need for Christians to bring their perspectives into the health sciences as an offering of hope.
He met with CHRISTIANITY TODAY to talk candidly about the Baby Doe provisions and to discuss the ramifications of Baby Doe dialogue on abortion, technology, and medicine’s own shifting ethic in the maintaining of life.
Part One: Baby Doe And The Mandate To Save
The Baby Doe provisions have now been signed into law by President Reagan. Specifically, what do you, as a physician, have here in the way of guidelines for handling Baby Doe-like situations?
Most obvious, I guess, is the fact that the law makes it a criminal offense not to treat certain infants, except in those cases where the infant’s condition would make any type of medical treatment futile or where treatment would simply prolong the death process.
Beyond that, the provisions call for the establishment, within a year’s time, of some sort of societal-based committee structure to review medical decisions in these “Baby Doe” cases. This aspect of the new provisions is also controversial. The AMA [American Medical Association] especially sees it as taking away the right of a doctor and family to make medical decisions and putting those decisions in the hands of people who will have all of the authority but none of the responsibility.
We’ll address these ethics committees in a minute. But for now, you’re saying—or I should say, the government is saying—that there are certain situations where nontreatment will be legally allowed?
Yes. And obviously that’s a problem for many people. Certain right-to-life lobbies, for example, walked out of the negotiations on these guidelines because there were occasional cases where nontreatment would be allowed. We physicians, on the other hand, now find ourselves legislatively dropped into something of a grey medical/legal chasm—left relying upon ourselves, these committees, the specific situation—in formulating the distinctions between when and when not to treat.
How do you as a physician and as a Christian draw those distinctions in your own mind and practice?
It’s not a decision that any of us feel comfortable with. And for the Christian physician, it’s hard to make a decision not to treat, whether we’re dealing with infants or terminally ill adults.
When I was in medical school, my first patient had amyotrophic lateral sclerosis (ALS)—Lou Gerig’s disease. He had pneumonia and his breathing was labored. It was near the end for him. He wrote us a little note—which makes it different from the nursery—that said, “Do not resuscitate.” That night he had a cardiac arrest. The physicians in charge at that time did not know him and they rushed in to resuscitate and put him on a respirator. He survived the attack. The next day we came in and found out what had happened.
As we stood by the bed of this business executive whose mind was still excellent but whose muscle and organ functions had totally deteriorated over the last three years, he took a piece of paper and, with tears running down his eyes, just put a question mark on it and pointed to the respirator. We as physicians remember those things. We don’t forget them.
If possible, there are times when we will keep a severely handicapped newborn alive for two or three days to allow the family to bond with that infant; to give the family an opportunity to express the love that is essential at any birth; and to give the family the opportunity to express sorrow so that it might be temporal and not come back to haunt them years later. But to prolong an agonizing, painful situation for two, three, or four days for the sake of some group’s political agenda is inhumane. It’s not a loving, compassionate approach toward either the child or the family.
Is that a Christian approach?
I don’t know. Sometimes I wonder. I think it is.
What makes you think it is?
Well, the Sermon on the Mount is a very motivational approach to ethics. Then you move into Colossians 2 and 3, where Paul is talking about do’s and don’ts, and he seems to be saying that ethics is not constant rule making but an understanding of what Christ would have you do in an individual situation. We therefore get to a deeper level than saying, “All babies should be resuscitated and put on respirators.” It becomes a motivational response to individual situations. There will always be an occasional difference in the way you handle one infant from another. And, yes, I think that is within the New Testament ethic as I understand it. But, it does leave a hole for people to be abusive.
After hearing what you’ve just said, a right-to-lifer would say you’ve been abusive toward life.
I know that, and yet I consider myself prolife. It saddens me because I feel that at the base of the right-to-life movement is the same religious understanding I have. I value man because of the value placed in man by God—and because I value God. My love for God through Jesus Christ means I will do everything I can for my fellow man. I think the right-to-lifer feels the same way. I think the distinction comes in our viewpoints. As physicians we deal with specific situations that can no longer fit into someone’s overriding rule and still be compassionate to the neonate or that businessman dying of ALS.
And yet, right-to-life groups are outspoken advocates of the sanctity of life?
Right. But their rhetoric is, at times, too extreme and, consequently, is ignored by many within the medical community. I can’t tell you how upset and angry disability groups were over their attempt to heighten public awareness of Baby Doe situations by putting out Baby Doe candy bars, T-shirts, and license plates. For them to feel that callously about our children really upset us, and we began to realize that their concern was not our children as much as it was an issue. It drove a wedge between disability and right-to-life groups.
Part Two: Baby Doe And The Abortion Question
In his controversial book, Brave New People, D. Gareth Jones describes the fetus as a “potential person.” Many people have a problem with that.
I do too.
Why?
We don’t treat the fetus as a potential person. We have been approaching the fetus as a patient for a long time, especially in the third trimester when it is still a fetus. We can do a lot of things for that fetus that basically elevate it in every way and every sense to personhood. We operate for the benefit of the fetus—we do it every day. We monitor the fetus—we do it every day. We intervene when it appears ill and rush in to save its life. And I mean we rush. It’s a two-minute dash to the C-section room to get out a fetus who has collapsed its cord. It’s a dash for a life we feel is very, very personal. So, to say that the fetus is only a potential human life is to miss some of the quality that we have already placed in it.
What impact has Baby Doe and its resultant legislation had on all this?
As I’ve said, we have already begun to view the fetus more as a patient. Baby Doe legislation enhances that view—makes it more substantive and gives it more backing. What we’re looking at now is a situation where the American public has very vocally said that they want medicine to show positive values toward handicapped newborns. Once we have said positively that we want to support handicapped newborns, critically ill newborns, it’s going to be very difficult to support a handicapped newborn at 25 weeks and yet say we can destroy it in utero one day or one week earlier with an abortion. Complicating this, if you will, is the fact that the fetus has an opportunity to survive much earlier outside the womb. And this, of course, further blurs the whole concept of viability.
Wasn’t viability—or the fetus’s ability to survive outside the mother—a key factor in the Supreme Court decision legalizing abortion in Roe v. Wade?
Right. With our intensive care nursery system now, newborn babies that were repeatedly written off a few years ago are now surviving. A baby of one pound has an opportunity to live today—something unheard of five years ago. And I think technology will soon take us to a point where a baby outside the uterus can be supported at almost any gestational age. That’s going to mean that society will have to deal with a technology challenging its values. It will mean that abortion without a medical reason is going to become more and more problematic for society.
Remember, without a reason to do something, medicine is usually loath to do it; in every operation, we demand conscientious decision making. Then the abortion issue came along and suddenly we said, “Reasons are not necessary. It’s whatever the mother desires. It’s her life, and she can exercise her automony.” That goes against the grain of even the American College of Ob/Gyn and its statements in the seventies about abortion. They demanded that physicians not be technicians, that they continue to have a value system, and that they continue to exercise their reasoning ability on a patient-by-patient basis. This is the second major impact of Baby Doe on the abortion issue. Adult autonomy is no longer viewed as an absolute by a society demanding societal review of certain life-and-death decisions.
Doctors are opposed to performing abortions?
I don’t know if I can speak for all of them. But I do know that many physicians generally are more bothered by social abortions or convenience abortions than almost any other procedure. Still, I must speak frankly and say that they would also be bothered by a sweeping law that never allowed an abortion. I think most physicians, even those of us who would like to see more reasonableness return to the abortion scene, would probably be bothered by that.
I couldn’t do an abortion unless I thought the life of the mother was going to be lost. I’ve been in two situations where we all felt that way very strongly, and we intervened. I have no qualms about it, have no guilt problems with it. I would do it again, given the same situation.
People ask me about rape and incest. I have trouble with it. Is the functional life of a mother going to be lost by giving birth to a child out of rape or incest?
What about the child born without a brain, the anencephalic?
To force a mother to carry that anomaly is almost inhuman. Let me give you an example. I know of a patient who had recurrent anencephalic babies. In those years and in this particular situation, federal funds were cut off for all abortions, therapeutic or otherwise. When she was pregnant with an anencephalic child for the second time, the physicians in charge tried to get an abortion okayed for her at government expense and couldn’t. She had the baby and did everything she could to adjust—even taking the baby home with her to die.
Her third child was also anencephalic. She had wanted an abortion and was almost desperate for it. But again, that was out of the question. She had the child and took the baby home to die. She then spent the next several years in and out of mental institutions. I think there is something of a cruel nature in that. And I think that that is an indicated abortion.
Part Three: Baby Doe And Modern Technology
You said recently that the supportability of amniocentesis—the procedure of extracting amniotic fluid from the mother’s womb—is questionable in light of Baby Doe. What do you mean by that?
It’s a good question because of the technological advances of amniocentesis and prenatal genetics sampling and counseling. As I mentioned earlier, the Baby Doe situation and debate have brought about a new positive attitude toward handicapped newborns. It is really difficult for the obstetrician to have a positive attitude about a handicapped newborn and a thoroughly negative attitude about a handicapped fetus, when there may be only a few days separating the one from the other. So this is a situation where our amniocentesis counseling may need to be altered. And not just our amnio counseling, but counseling done as a result of chorionic villus biopsy as well.
Is that something new?
Yes, it’s something new in our country and, in fact, it hasn’t been approved yet. Basically, it will allow us to determine chromosomal anomalies and a number of other things, all within the first trimester. Of course, the problem here, again, is selectivity. Suddenly we will have a tool that will allow people to select “the right child” all within the first three months of life. They may select out male versus female. Or they might want to select out any number of recognizable disabilities that have nothing to do with mental retardation or even a severe physical handicap. Baby Doe calls all of that into question simply by saying that handicapping conditions cannot be a reason to eliminate life once it is born. It asks pointedly how much concern we really have in our society for “the least of these.”
So counseling becomes a delicate matter?
Yes. Unfortunately, the obstetrics counseling involving amniocentesis has rarely been what I would term appropriate. Most of the counseling is extremely negative. It is usually something that’s overly simplified, like, “When you’re over 35 you have to have amniocentesis.” Many times when a patient refuses amniocentesis, she’ll be asked to reconsider two or three times. You know, “Are you sure you don’t want amnio? You’re 40 years old. You’re a risk. There’s almost one Down’s birth in 20. Are you sure you don’t want amnio?”
It’s negative counseling. And the problem is, our legal system protects such negativism. The physician doesn’t feel free to give both sides of the Down’s syndrome story. If he is ever found guilty of talking someone into having a child with Down’s syndrome, he would also be found medically and legally liable for that child. So the courts have said that if a physician ever coerces or in some way allows a birth to occur that could have been eliminated, and by standards of practice should have been eliminated, then he is medically, legally, and financially liable for that child. And that’s a significant problem to overcome in trying to change any of the counseling methods in the prenatal period for amniocentesis.
How do you feel, then, about amniocentesis?
That’s a hard question. I used to feel good about it. I felt that if there was any way we could prevent the arrival of handicapped newborns, we should do it. That sort of thinking is ingrained in you as a medical student. It’s a given. Well, I have trouble with the basic principle. We look at our own child, Ginny, who has Down’s syndrome, and see our own limitedness. She shows us love even when we, at first, were not totally accepting of her. These kids love us until we begin to love them back. And by loving them, we learn a whole new definition of love—something very akin to grace.
In our country we have been very much aware of physical attributes and their importance in being successful. But with a child like Ginny, we learn that love is deeper. It’s love because of the personal qualities of that child and because of something of the spirit of God that’s within that child—what we term personhood.
So now that we have had Ginny, amniocentesis is somewhat threatening to us. It threatens something of the love that we have learned to express for our child. It’s no longer something I can look at with such lethal abandon. I think it has its place. When it leads us to severe hydrocephalus or anencephaly in the midtrimester, those are essentially untreatable situations; even with current technology. But I have trouble, at this point, with amnio aimed at destroying all handicapped newborns before they are delivered.
So how do you, as a Christian physician, ultimately deal with such technology?
We can go one of three ways. One way is to be so limited in your ethical and moral viewpoints that nothing is allowable, technologically speaking. That’s like ignoring the rain that’s already fallen upstream. You eventually find yourself in the flood you said wouldn’t happen. If you are unable to reasonably discuss what has already occurred, your voice will probably not be heard.
The second way is to take the course medical ethics has been accused of taking over the past 20 years—that is, be so broad, so laissez faire in your viewpoints, that anything is okay and any kind of medical technology is fine. But this, too, is meaningless.
The third way is the challenge facing any Christian wanting to enter the medical fray. We must learn to bring Christian values into the systems that are with us here and now. We can’t go back to the year 1200. The Lord has allowed us to develop the technologies of today, and it is our responsibility to use them in a framework of Christian principles.
Part Four: Baby Doe And Medical Ethics
Earlier you mentioned ethics committees as part of the new Baby Doe provisions. Why are such committees even necessary?
Partly because physicians have not consistently provided accurate counsel regarding the quality of handicapped life, and partly because of the psychodynamics at work in these situations. The overriding impact on the family, in terms of medical decision making, is the problem of ambivalence. You love the newborn because it’s alive and our culture says you love live newborns. There is also that incredible sense of loss of the child you wanted, the child that did not arrive. You basically have to work through the death of that child. You agonize over the self-image that is now destroyed. So in between the need to be positive and the agonizing negative sense of loss is an ambivalence that makes it very difficult for a parent to make rational decisions. To maintain that they have total discerning capabilities at that point is unreasonable.
That’s a horrifying thought. I would hate to think that if a child of mine were born handicapped, I would be considered incompetent to make a decision regarding treatment.
Here we get to the ideal function of these ethics committees (which, by the way, will not be completely spelled out for some time). Generally, it will be to make sure that all the facts in a given situation are properly considered before a decision regarding treatment or nontreatment is made.
It seems to me that ethics committees should have as their primary aim the creating of a nurturing environment for the newborn. And the only way they are going to do that is to help the parents begin to understand and deal with the newborn and, if at all possible, accept that newborn. Without this, we are going to have more Indiana decisions, more court cases, and more public debates that are going to upset a large number of Americans.
Under whose ethics will these committees function?
First of all, the good thing about ethics committees is that they imply several things to the medical community. They imply that serious consideration is being given to each situation; they imply that issues are being discussed, that every type of helpful consultation is being sought, and that each decision is being made jointly between people who care. That’s what ethics implies to a large number in medicine—and those are wholesome qualities.
Neither government nor I like ethics when it brings in all kinds of social, economic, and philosophical concerns that take your interest away from the infant. Suddenly, you’re working in the best interest of society; you’re working in the best interest of some economist who says we’ll go broke in five years if we save the baby’s life. If these committees are going to function in a Christian, ethical fashion, they must discuss “whys” over “hows”. They must discuss motivations over procedures, and concentrate on what is in the best interest of the newborn child.
Do you sense that the medical community is more willing to consider an ethical view based upon a more traditional or, if you will, more Christian perspective?
Yes. There is a desire to get back to traditonal values. It’s almost an urgency. Of course, they’ve sought ways to make those traditional values nonreligious. But the Christian person, and I as a Christian physician, looks at that and says we’re offering traditional values grounded in the concept of a faith that has been lifesaving for centuries. We know these values are workable, are usable, and that they are positive because of their legacy of changed lives.
In the future, physicians will face a problem in giving informed consent on so many new technologies and methods. For instance, when using the new reproductive technology they will have to inform people about the ethical as well as the medical problems in each situation. Physicians will need to be in touch with traditional values because their patients are. If we refuse to recognize them, it will create more problems for us than we have now. So, there’s a practical reason for returning to traditional values—but there’s also an urgency within the physician to understand them better.
That should bode well for the sanctity of life?
I think so. There are three medical values that have been undeniable down through the centuries. One is that medicine has had a radically positive view of man. Man is worth saving, is worth treating. He is worth enough to have other men and women—doctors—work night after night after night away from their families and in the constant threat of malpractice suits.
Second, medicine has traditionally viewed suffering within man as something meaningful. It’s not merely disease or pain; it’s more than that. Finally, medicine has had a tradition of emphasizing the personal, covenant-like relationship between doctor and patient. One of promise and fulfillment. One of sacrifice and serving.
Many say that these traditions have been lost over the past 15 to 30 years. Many say we no longer view man as positively as we should, and that we have allowed abortion laws and things of that nature to erode our value of man. Many say we no longer view suffering as something meaningful because we are too tied up with technical approaches to suffering and overspecialization. Finally, many say the contract relationships and businesslike, profit-oriented practice of medicine have destroyed the covenant relationship that was in our ethical approach for centuries. Thus, what we see today is an urgent need on the part of physicians to return to those traditional approaches of medicine. And yes, it does underline a sanctity of life view, it does underline a personal relationship view, and a covenant view that has deep theological roots. I think we will be reaching a time very shortly when theology and medicine will be closely tied again—as it once was—at least in the minds of many physicians and patients.
So you’re optimistic about the future?
Yes. Maybe that sounds crazy, but I do. It’s like reading the Book of Habakkuk. If the last four verses in that book were missing, what a tragedy life would be. We’ve all stood there and screamed at the sky and said, “When’s this going to stop? When is something going to work here?” There are answers; there is hope, and hope lies within our ability as Christian people to keep in touch with God through a personal relationship with him. He allows us to be optimistic. He allows us to hope.
CHRISTIANITY TODAY talked with the following individuals to get some of their own thinking regarding Baby Doe and his impact on medical and societal ethics and decision making. Using the Elkins interview as a starting point, they offered these brief insights.