As I lay in a hospital bed, the doctor and I tried to figure out why red, purple, and blue patches were erupting all over my body. My blood platelet levels were so low, I could have developed spontaneous internal bleeding. ER residents crowded into the room, curious to see my skin. We went down the list of potential causes: a family history of bleeding disorders, recent medication exposures, cancer symptoms, recent infections.
Then I remembered. Three weeks prior, I had received several vaccines to prepare for a medical missions trip. As I endured much testing over the following weeks and years, only one explanation persisted for my immune thrombocytopenic purpura (ITP): A vaccine had tricked my immune system into attacking my own platelets, the parts of blood cells that bind them together.
I know the risks of vaccines quite intimately. Even so, I continue to take vaccinations, I ensure that my children get them, and I recommend them to all my patients. Before becoming a family doctor in Baltimore, I studied immunology in medical school, learning how and why vaccines work in order to offer them to my patients. Like all parents—including, of course, those who refuse vaccines—I want what’s best for my children. As I have thought about my own story and studied vaccines, I’ve grown confident in this: The benefits of vaccines are far too great for us to refuse, and the risk of refusing them extends far beyond our own families. This is not just a medical issue, but an issue that touches on our faith and our public witness.
The Worry Over Vaccines
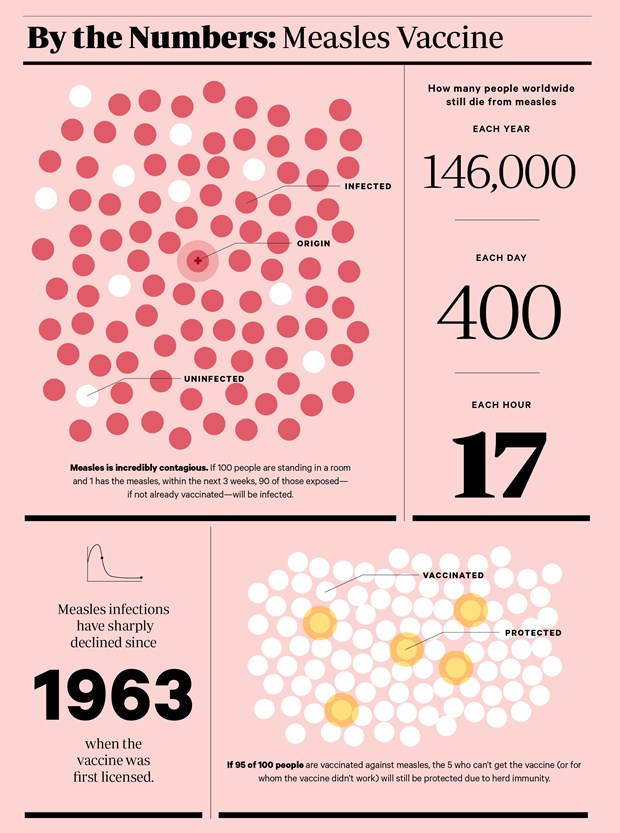
In recent years in the West, including among Christians, concerns about vaccines have grown, leading to measles outbreaks in pockets of the United States and in Germany, where an infant died of the highly infectious disease this winter. Vaccination rates are so low in some states, some wonder if we’ll lose herd immunity—the protection given to a population when so many people are vaccinated that a disease can’t spread, even if the vaccine isn’t effective for everyone.
Yet many parents still believe vaccines’ risks outweigh their purported benefits.
Members of the antivaccine movement note that many vaccine-preventable diseases were on the decline before vaccines were widely used. This is true (in some cases, anyway) largely due to improved medical care across the board. These prevaccination declines underscore that health is not simply about following the medical industry’s recommendations. More broadly, health means a whole community practicing a range of behaviors and making structural developments (mostly related to sanitation) to see general health improvements.
Here we can learn from communities that deliberately choose not to vaccinate. Their focus on individual health, an unpolluted environment, and the tight community bonds that allow them to propagate their ideas make them less likely to suffer from heart disease, cancer, and other illnesses that kill far more people in developed countries than vaccine-preventable diseases do. Families that breastfeed, exercise, avoid junk food, opt out of daycare, and follow a more “natural” way of life are indeed less susceptible to disease. So why, they reason, put a mixture of foreign DNA and artificial chemicals into a child’s body to prevent those diseases?
Further, families who reject vaccines note that materials used to make them—such as mercury and aluminum—could harm our bodies, particularly our brains. Christians and non-Christians alike argue we were created with immune systems designed to ward off disease, making “artificial” prevention obsolete.
Some Christians in particular are concerned that vaccines are made using cell lines taken from unborn babies aborted decades ago. The cell lines are manipulated in a lab to divide indefinitely, providing a medium in which to grow a weakened virus. These Christians worry that getting vaccines amounts to cooperating with evil, especially given that research on aborted fetuses continues today. (For example, neuroscientists have transplanted cells from aborted fetuses into the brains of people with Parkinson’s disease.)
In sum, vaccine critics note that vaccines have no obvious benefit while posing health risks, all while participating in a potentially murky ethical system. Add to this the powerful stories from individuals whose children developed debilitating diseases after getting vaccines, and the no-vaccines case seems strong.
The Power of Stories
But as compelling as that case may be, it ultimately doesn’t grapple with how we as a society measure health benefits and risks.
Let’s first clarify the language we use to talk about medical intervention in general and vaccines in particular. All medical interventions—whether a simple cholesterol test or a complex surgery—carry both an increased chance of benefit and an increased risk of harm.
Article continues below
If you have pneumonia or a blood infection, a doctor will prescribe an antibiotic as a treatment that carries side effects. But the risk of the infection is higher than the risk of the side effects. Therefore, the antibiotic is a wise medical intervention. By contrast, antibiotics do nothing to kill viruses that cause colds, and also introduce unnecessary risks. Many Westerners request antibiotics for these viruses because they want to relieve their symptoms. But in this case, an antibiotic is a poor medical intervention and should be avoided.
We’ve all seen the TV commercials for new drugs that purport to treat one ailment while potentially creating dozens more. These commercials demonstrate that no medical intervention is completely free of risk—and some, like the antibiotics used for colds caused by viruses, create a greater chance of risk than benefit. Further, the medical community has notoriously overprescribed an enormous variety of drugs. We’re wise not to assume that a medical consensus always implies scientific rigor. It doesn’t.
But we’re also wise not to assume that individual stories—which are as powerful as scientific research in shaping public opinion today—have the final word. Even I can’t say for sure that a vaccine caused my autoimmune disease. We can’t ever let a story or set of stories, no matter how compelling, negate a larger body of evidence about how well a treatment works or how frequently it harms. This is especially true when discussing what’s best for a whole society.
When I had ITP, I was bruising for two weeks before I sought treatment. Knowing that I’d recently received vaccines, I figured that I’d had an innocent drug reaction and continued on with my 14-hour workdays. By the time I saw my doctor, she took my otherwise normal appearance as a sign that I’d be fine. Then she ordered a battery of tests to figure out what was going on. Two days later, I got the call that my platelets were critically low and I needed to get to the ER immediately.
I had misidentified my rash, and my doctor had overlooked its seriousness. That I actually felt fine didn’t help: it prevented me from seeking care sooner and prevented my doctor from acting faster. I had just enough knowledge to take serious risks, such as riding my bike and playing Ultimate Frisbee.
Similarly, if our decisions about vaccines are based on how healthy we feel right now and how infrequently we get vaccine-preventable diseases, we’ll miss the big picture of how dangerous these diseases can be and how powerful vaccines are. We can avoid this error by sifting through as much information about vaccines as we can and basing decisions on the studies with the largest numbers of participants, putting less weight on individual anecdotes. So let’s look at the largest studies.
Article continues below
The Big Picture
When it comes to the measles, mumps, and rubella vaccine, a combination of studies involving millions of subjects find that the chance of benefit is incredibly high. This has translated to ever-decreasing rates of measles, mumps, and rubella, along with decreased death and disability from these diseases, worldwide. Meanwhile, the risk of harm is demonstrably low. About one in six children have a low-grade fever or rash the day of the shot. Seizures resulting from a fever—which are scary but harmless—occur generally at rates of 1 or 2 per 1,000 vaccine doses.
More serious reactions (such as thrombocytopenia, which is similar to ITP) occur less frequently. Even then, they are still less frequent than complications brought on by measles, mumps, or rubella. And when the risks of a vaccine outweigh the benefits—such as in the case of RotaShield, meant to treat diarrhea in young children—public health officials usually step in to pull the product.
What about those artificial components? Aluminum and formaldehyde occur naturally in our bodies or in the environment at concentrations higher than those in vaccines. Research continues to demonstrate that an infant’s body can safely handle the amount of aluminum found in vaccines. In the case of autism, studies with larger and larger sample sizes demonstrate no link between autism and vaccines, despite otherwise compelling stories from individuals who see a connection between the two.
The scientific evidence overwhelmingly suggests that vaccines carry a high chance of benefiting us and an incredibly low chance of harming us. The more effective a health intervention is in saving lives, the more morally responsible it is for a community to promote it.
Still, many Christians are rightly concerned that some vaccines are made using cell lines from aborted babies. To be clear: We should oppose any ongoing research that treats a vulnerable human life so callously. And, as the Catholic Church suggests, all Christians should implore pharmaceutical manufacturers to find vaccines without such tainted histories wherever possible.
Article continues below
Even so, getting a vaccine that includes components produced by these cell lines doesn’t causally cooperate with evil. Indeed, it’s nearly impossible to do anything without cooperating, however distantly, with evil. As the Southern Baptist Ethics and Religious Liberty Commission noted, getting a vaccine that uses these cell lines doesn’t fuel the number of abortions; likewise, avoiding such vaccines doesn’t prevent abortions from happening. There are far more effective ways to advocate for the lives of the unborn—ones that don’t pose a health risk to us or our neighbors.
How, then, to think about vaccines from a biblical perspective?
Health Is Stewardship
First, we have to understand health not just as the absence of disease but as wholeness in our bodies and communities. It’s what the writer Wendell Berry has called “singular integrity and communal belonging.” From this perspective, health means stewarding all the resources God has given us to bring about human flourishing and full image-bearing among our families and neighbors. Preventing the most deaths for the lowest cost with the simplest interventions is a core part of stewardship.
We find an example of this stewardship in the Old Testament. Reflecting an early Judeo-Christian vision of “public health,” the Levitical law prescribed quarantining people and property with infections that could spread to others (Lev. 13). Landowners were held responsible for injuries incurred on their property (Deut. 22:8) or by their animals (Ex. 21:28–29). Our relationship to the natural world is one of stewards; to each other, as image bearers and, among Christians, coheirs with Christ. This means we make use of every morally sound means to promote health for all.
Considered in the wider context of stewardship, there is no coherent biblical reasoning that discourages us from putting anything “artificial” in our bodies. The distinction between the “natural” world and the “artificial” one has been blurred ever since humans started planting crops in rows instead of scattering seed. Even those who practice the healthiest lifestyles to prevent hypertension, diabetes, asthma, and cancer are not fully protected from these maladies. Many require lifelong medical treatment—in tandem with a healthy lifestyle—to reduce disability or prevent early death. By giving our bodies just enough ingredients to develop immunity instead of waiting for disease to strike, we’re proactively conforming to a pattern of wholeness.
Article continues below
As vaccine skeptics point out, healthier children are less likely to suffer complications from vaccine-preventable diseases. Even so, a Christian vision of stewardship extends beyond the health of individuals or families. As essayist Eula Biss notes in her book On Immunity, humans are prone to clutch at control to the point that the artificial ingredients in vaccines terrify us more than the diseases they prevent.
Protecting the Vulnerable
Many are not so privileged as to opt out. Those who suffer from poverty or immunosuppressive disease do not have the same power to protect themselves and their children. Parents who consider the effects of vaccines only on their families without considering the wider consequences are, from a public-health perspective, whittling away at the herd immunity that protects the most vulnerable. It’s like a town that lives at the source of a river and disposes of their waste in the water—forgetting the other town downstream. Not vaccinating elevates the risks of infectious disease among the poor and immunosuppressed.
From a global perspective, the problem is more acute. Previous generations bore the risks of smallpox vaccination. Now the disease is eradicated worldwide, and the vaccine has saved millions of lives. Polio may be the next breakthrough, as researchers estimate that millions have dodged lifelong paralysis or early death. While efforts to ensure appropriate sanitation and nutrition are a priority, vaccines still represent a crucial weapon against diseases that would otherwise kill many.
This reasoning applies even to diseases typically spread through unprotected sex or drug use. The hepatitis B vaccine, for example, was initially focused on “high-risk” populations. Then researchers realized a small number of children were getting infected without engaging in such behaviors. Since universal vaccination at birth was started, the incidence of hepatitis B has declined dramatically.
We can celebrate that God has mercifully given us insight into how the human body and the diseases that ravage it work; because of his mercy, we can exercise dominion over the natural evils of disease. Genesis 3 teaches us that since the Fall, creation naturally bites back at us through thorns and viruses as part of God’s curse for our sin. Yet we who have been redeemed partner with God in his work of redemption, in part by fostering our communities’ health.
Article continues below
It’s no surprise that medical missionaries have played a crucial role in advancing health care across the globe over the past several decades. They carry Jesus’ mission to preach and heal in places that desperately need all kinds of healing.
Immunity and Eternity
As a medical student, I started by learning about anatomy and physiology. Then I learned about infectious disease and pathophysiology, then pharmacology and therapeutics. The curriculum’s structure is a reflection of how medicine is meant to work. The practice of medicine explores the body and its functions in their original goodness; identifies patterns of decay brought by sin; and works to undo or prevent those patterns from harming our bodies and minds.
And we practice medicine expecting that our present bodies will be raised to new life. Paul writes in 1 Corinthians 15, “The body that is sown is perishable, it is raised imperishable,” like seeds bursting into full-grown plants. As Matthew Lee Anderson writes in his book Earthen Vessels, “The same God who forgives sin shapes and reshapes human bodies.” Thus, all of our medical care and healthy behaviors still rest on God’s mercy, and they anticipate that complete healing will come not in this life but in the life to come.
Even still, we can take all the precautions prescribed by the best science and fall prey to an infectious disease (or suffer a horrific side effect). We can refuse all vaccines for our children and still watch them suffer neurodevelopmental disorders. While science and medicine help us to decrease risk, there’s nothing any of us can do to stop death. When we perform medical interventions, then, we must humbly acknowledge that we can never guarantee a particular outcome. Nor should we ever forget that God can and does use supernatural means to heal. Medicine, rightly practiced, recognizes that our bodies and our souls are marred by sin but that God will one day restore both. We carry on the work of Jesus, knowing that one day the work of both evangelism and medicine will come to an end.
Three days before I was admitted to the hospital with ITP, I got whacked in the head by a Frisbee that left an enormous bruise behind my ear. I thought about that a lot sitting in the hospital, watching my brother get married over Skype and forgoing the best man speech I’d prepared, and emailing the mission hospital where I had planned to work. I was alive now. But would my body recover from this side effect? Would I ever get to go to the mission field to preach and heal, as I felt God had called me to do?
Article continues below
I’m happy to say God has seen fit to restore me to health. At the end of this year, our family will travel to South Sudan, one of the world’s deadliest places, to work in a maternity and pediatrics hospital. The risks we’ll face—poisonous snakes, tropical diseases, political violence—are quite real. I can’t guarantee that my disease won’t relapse at a time when I’m far from a platelet transfusion. Nor can I guarantee that one of my children won’t develop a problem with catastrophic consequences.
Yet the same God who protected me from serious injury is beckoning us there. We trust that he will take care of us. We recognize that our lives—and our children’s—are in his hands. These are risks he has called us to bear for the sake of his glory and love. We can maximize our effectiveness there by counting the cost, but we cannot cultivate health by magnifying our anxieties to the point that they obscure the value of the gifts he’s given. God has called us to steward wholeness in one particular community. The benefits that we’ll see and that the people we’re working with will experience as his kingdom advances far outweigh the risks of going.
Of course, for our sake—and for the sake of those we meet both abroad and back home—we’ll be getting our shots before we go.
Matthew Loftus is a family doctor based in Baltimore who writes regularly at the blog Mere Orthodoxy. Follow him on Twitter @matthew_loftus.
Image: Data • Centers for Disease Control
Have something to add about this? See something we missed? Share your feedback here.















 While we pray for peace, we need moral clarity about this war.
While we pray for peace, we need moral clarity about this war. A Christian reconciliation group in Israel and Palestine warned that war would come. Now the war threatens their relevance.españolالعربيةFrançaisрусскийУкраїнська
A Christian reconciliation group in Israel and Palestine warned that war would come. Now the war threatens their relevance.españolالعربيةFrançaisрусскийУкраїнська The rage of the mob is a poor substitute for real community.
The rage of the mob is a poor substitute for real community.
